






COVID-19: Why is WHO’s Tech-Sharing Platform C-TAP a Non-Starter?

Representational use only.
Even a year into its launch, the COVID-19 Technology Access Pool (C-TAP), a global platform to share technology on COVID-19, has remained a non-starter.
Meanwhile, the world has become divided into the vaccine haves and have nots. A failure to get the C-TAP going has resulted in the emergence of a vaccine disparity between rich and poor countries. In most of the low and middle income countries, the proportion of fully vaccinated population is much less than in the rich countries. The rich countries such as Bahrain (46%), the United States (40%), and the United Kingdom (38%) have been able to fully vaccinate a sizeable proportion of their population, while in the entire African continent only 0.6% of the population has been fully vaccinated till May 30. How did this happen?
In March, 2020 Costa Rica mooted the proposal for C-TAP and the Solidarity Call to Action “to realise equitable global access to COVID-19-19 health technologies through pooling of knowledge, intellectual property and data”. Subsequently, the C-TAP was launched by World Health Organisation (WHO) in May 2020. It aimed at improving equitable global access to COVID health technologies through voluntarily pooling knowledge, intellectual property and data to support technology transfer and rapidly expand manufacturing throughout the world.
There are 42 countries which have joined the initiative, with Spain being the latest. Notably, none of the countries which have the manufacturing capacity and the know-how, and which host big pharmaceutical giants have signed up, and these include the US, the European Union and even India.
None of the vaccine-producing Pharma companies have joined the initiative as they are concerned about protecting their trade secrets and monopoly over technology. Another patent sharing platform, the medicines patent pool (MPP) has also not seen any deals negotiated for drugs, data or technology to fight the pandemic. In fact, the Pharma lobby has been snubbing the C-TAP initiative as being “nonsense” and “dangerous.” Instead, the Pharma companies have been putting their weight behind the The Access to COVID-19 Tools Accelerator (ACT-A) , launched in April 2020 at the behest of the Bill and Melinda Gates Foundation, CEPI, GAVI and other such global platforms partial to protecting intellectual property rights.
Concentration of Manufacturing Capacity at a few Centres
Underlining the need for enhancing the manufacturing capacity many fold, Okonjo-Iweala, the WTO Director General, pointed out that Africa has only 0.2% of the global production capacity while Latin America has just two per cent. The D-G said: “In the longer run, especially if COVID-19 is with us for years, we need a more geographically diversified global vaccine manufacturing base”.
According to the WHO Global Vaccine Market report, 2020, vaccine manufacturing remains concentrated with four large manufacturers (Glaxo Smith Kline, Pfizer, Merck, and Sanofi), controlling 90% of global vaccine value, and five producing 60% of global volume (Serum Institute of India, GSK, Sanofi, Bharat Biotech and Haffkine). Although during the COVID-19-19 pandemic, China has emerged as an important global player, but its human vaccine market has largely been occupied by local companies, not occupying much significant share of the global market.
Concentration of the production capacity in a few locations across the world, such as the Serum Institute of India (SII), and the Modi Government’s inability to boost up and use local capacity to produce vaccines has resulted in miscalculation in the supply of vaccines not only in India, but with implications for many other countries. Left in the lurch, most poor countries had to eventually look towards China and Russia for their vaccine supplies.
On the occasion of the first anniversary of the C-TAP, in a media briefing, the WHO member states reiterated the need for technology transfer to boost up vaccine manufacturing across the world. The Indonesian Health Minister stated that the country has six manufacturers with a production capacity of about 550 million doses per annum. Abdul Muktadir, Chairman of Incepta Pharmaceuticals, Bangladesh, echoed the need for technology transfer and asserted that there are untapped high quality production capabilities in countries such as Bangladesh.
In the press briefing, Mariangela Simao, the WHO Assistant Director General for Access to Medicines, Vaccines and Pharmaceuticals, acknowledged that there is a “huge capacity out there” in the developing countries. She expressed that there is an interest from the countries in receiving technology, and with a strong support on local production resolution being discussed at the WHA (World Health Assembly), this is the time to understand the urgency of C-TAP. She informed that C-TAP is in discussion with two vaccine manufacturers which may be willing to share technology.
In a statement Health Action International (HAI) said that “…the high expectations of C-TAP to halt the global catastrophe as it unfolds, have not been realised. This is largely down to the refusal of the pharmaceutical industry to engage, preferring instead to protect short-term profits over global public health.”
Did ACT-A subvert C-TAP?
It was soon after the proposal by Costa Rica for the launch of a platform such as C-TAP (in March) that the ACT-A was launched (in April). The ACT-A, a public-private partnership initiative is, in principle, rooted in a status quo vision for organising the research, development, manufacture, and distribution of treatments and vaccines. The experience over the past one year has shown that ACT-A conveniently overshadowed the C-TAP initiative.
The idea of ACT-A works by propagating the argument that intellectual property rights (IPR) must be protected, even during a pandemic, and that these are not a hindrance to meeting global demand or ensuring equitable access. The ACT-A, along with its vaccine arm COVAX, targets the development and distribution of vaccines for up to 20% of the population in Low and Middle Income Countries (LMICs). Effectively, after reaching this target the field would be left open to market forces. However, despite much fanfare behind the launch of ACT-A, and the ensuing commitments under ACT-A to ensure increased supply, vaccines are yet to reach most of the population in poor and middle income countries.
Despite tall claims made by the big pharma companies that they are committed to ensure increased and more equitable supply of vaccines, the lobby kept rejecting initiatives like C-TAP saying that IPRs are not the reason for restricted supply. In a statement International Federation for Pharmaceutical Manufacturers and Association (IFMPA) noted that they disagree with some of the premises of C-TAP, “as they imply that IPRs that are not waived or licensed globally are potential barriers to R&D, public-private collaborations or access to COVID-19 products.”
The tendency to maintain monopoly rights has been behind the reluctance to share the IPRs with manufacturers in LMCs. The ACT-A acted as a veil behind which the pharma lobby could continue enjoying unbridled monopoly power. The COVAX platform also focused on a few companies such as the SII. The ACT-A, thus, failed to increase vaccine supply and stark inequality emerged between the vaccine haves and have nots. It also successfully managed to sabotage the C-TAP. This has resulted in vaccine manufacturing being limited to a small group.
Within the ACT-A too, the bulk of the funding has been public. Out of the total funding of USD 15 billion, USD 13.1 billion is public funding contributed by various countries governments, USD 0.8 billion is from private donors such as the BMGF, Wellcome Trust and about USD 1.1 billion from multilateral donors such as the Global Fund and GAVI.
Concentration of Production Within Rich Countries
In a much-criticised remark made by AstraZeneca’s CEO Pascal Soriot, he said that AstraZeneca cannot share such technology with the WHO because it has no engineers available to assist in the technology transfer and stated that “the solution is to increase the yield in the existing plants, not to create more plants…”
In denying the transfer of technology to manufacturers in the poor and middle income countries, the pharma companies have completely disregarded the proven existing capacity in many of these countries in order to protect their monopolies.
A look at the manufacturing agreements between key vaccine producers and the manufacturers shows that the big pharma companies such as Moderna, Pfizer and Janssen largely have agreements with Contract Development and Manufacturing Organisation (CDMOs), with some being agreements being Technology Transfer (TT) agreements. CDMOs are companies which can contracted by the pharma companies to provide services from drug development to drug manufacture. Through these companies the pharma companies can outsource certain aspects of business to help with scalability. The agreements by these three pharma companies have been largely restricted to the manufacturers in the rich countries with a few of them being located in low income countries such as India (Serum Institute, Biologic E).
On the other hand, vaccine producers such as Gamaleya, Beijing Institute and Sinovac have largely entered into Technology Transfer agreements with manufacturers in various countries, which include the manufacturers located in the poor and middle income countries.
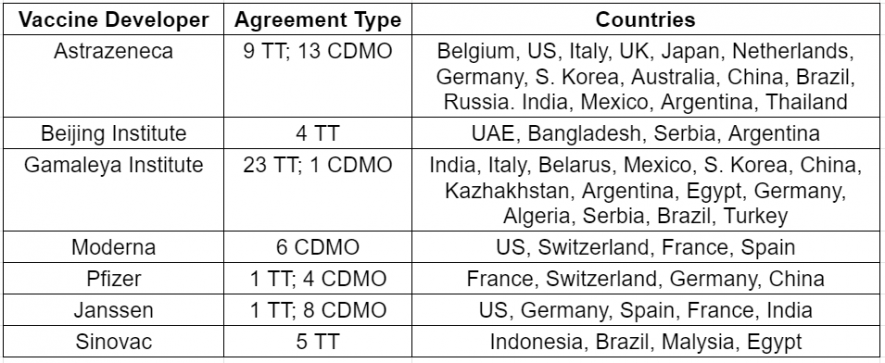
This clearly shows the skewed pattern of agreements that the pharma companies have been entering into. The agreements are largely with the manufacturers within the developed world, that too CDMOs, rather than technology transfers.
In a move towards more equitable and quick access to vaccines a global effort is required which is not driven by profit motive. The stance of the Pharma industry has been clear and sided with profiteering. It is now left to the collective efforts of nation states and international institutions such as the WHO to work towards ensuring global equity in vaccine distribution.
Get the latest reports & analysis with people's perspective on Protests, movements & deep analytical videos, discussions of the current affairs in your Telegram app. Subscribe to NewsClick's Telegram channel & get Real-Time updates on stories, as they get published on our website.















