






Lesson from Covid-19: To Avoid Catastrophes, India Should Adopt Risk Minimisation for All Policies

COVID-19 is a ‘gray rhino’--an event that is highly probable and with a large impact but it is neglected even though it can be seen well in advance due to its size and early warning signs. Now, over a year into the pandemic, India has remained completely unprepared for the COVID-19’s second wave.
India, like much of the world, did not foresee COVID-19 despite warnings and was caught napping. A dozen worldwide epidemics that occurred in the last century -- many with death tolls exceeding 1 million -- should have prepared the world for COVID-19, but their horrors faded quickly from public memory. World Health Organisation (WHO) Director General, Adhanom Ghebreyesus had warned the world in 2018 saying, “A devastating epidemic could start in any country at any time and kill millions of people.” However, the world was a sitting duck when COVID-19 hit in December 2019.
After the COVID-19 pandemic broke out in January 2020, the reported case load in India rose slowly and the first wave peaked by September 2020 at a shade under 100,000 new cases per day; then daily cases declined gradually to 10% of that figure by February 2021. This lulled the Indian government into believing that the worst was over.
In the last week of February 2021, as the second wave hit, the case load rose explosively in a near-vertical exponential curve. By early-May, over 400,000 new cases and over 4,000 deaths were being reported daily, i.e., 40 times greater than two months earlier. Bio-statisticians believe that these numbers are vastly under-reported, and that the real case load may be 10-20 times greater.
COVID-19 patients waited forever for ambulances, were put two to a hospital bed, and many simply died gasping for oxygen. India was down on its knees. Its COVID-19 plight, the worst that any country has faced, made world headlines.
The total reported COVID-19 deaths in India are now 326,000, and counting--the largest number of deaths to have occurred in a single disaster after the 1918 Spanish flu that killed 18 million Indians. How did India, a global pharma giant, suddenly find itself in such a dire predicament?
Deaths Due to I nadequate Public Healthcare Investment
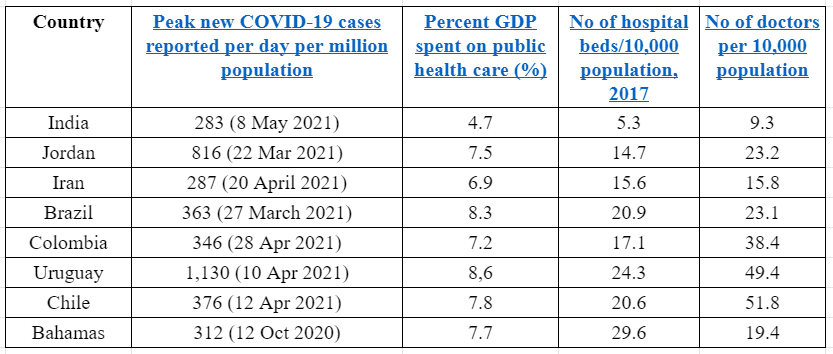
India’s woefully inadequate public healthcare system buckled under the relentless onslaught of COVID-19’s second wave. At the peak of this wave on May 8, 2021, India reported 283 new cases per day per million population. Other nations reported a similar incidence but did not face a crisis as they had invested more in public healthcare than India did. Jordan, Iran, Brazil, Colombia, Chile, Uruguay, and Bahamas had incidences ranging 287-1,130 new cases per day per million population. These countries invested 7-8% of their GDP on healthcare compared to India’s 4.7%. Consequently, they had 3-6 times the number of beds compared to India’s 5.3 beds per 10,000 population, and 1.5-5 times the number of doctors compared to India’s 9.3 doctors per 10,000 population.
Public health investment by various countries that have similar incidence of COVID-19
India’s modest boost to its health infrastructure after the pandemic broke out did not match the meteoric rise in the second wave’s case load. Data tabled by the government in the Rajya Sabha in February 2021 indicates that in the nine months between April 21 and January 18 in 2021, the number of oxygen beds, ICU beds and ventilators in the public health system increased by 152%, 32% and 80%, respectively. In this period, the number of active cases increased 12-fold (1200%), and if this period is extended to May 8, 2021, the increase is almost 250-fold. The current acute short supply of oxygen is not due to the lack of production capacity but the inadequate transport and storage infrastructure to send oxygen where it is required.
India’s high COVID-19-related mortality is due to the woefully inadequate public health infrastructure rather than the disease’s complications. Rural India, which escaped lightly in the first wave, is now being ravaged as public healthcare is scarce. Besides, India has gradually allowed quality healthcare to shift to the private sector, pushing it out of the poor’s reach. India failed to recognise that good public health care accessible to all is vital for its well-being.
India flying blind: Lack of transparency, zigzags moves
Scientists know that viral pandemics may have several waves. When harsh measures suppressing a pandemic wave are lifted, the virus again gathers strength, mutates sometimes, and hits back to cause the next wave. A vaccine, herd immunity or weakening of the virus are the only ways the virus is tamed. As happened in the Spanish flu, the second wave is often deadlier than the first.
On May 5, Vijaya Raghavan, Principal Scientific Adviser to the Government of India, stated that a third wave is inevitable, but two days later added that, “If we take strong measures, the third COVID wave may not happen in all the places or indeed anywhere.” Raghavan did not elaborate on the measures and how they would help avoid a third wave.
The government has not shared its understanding of the coronavirus’ transmission dynamics, which is the basis for pandemic management. Nor has it explained the logic of its zigzags moves—no restrictions till late-March 2020, then declaring the harshest possible lockdown, not declaring that India had moved into community transmission stage till date, declaring India’s victory over the virus in January 2021, holding elections in several states and allowing the hundreds of thousands of people to congregate in the Kumbh Mela in April 2021, then going into lockdown in many states this month. India has been flying blind in this pandemic.
Ignoring Gray Rhino Events May Give India New Name
COVID-19 is but one episode in a series of major hazard (cyclones, earthquakes, pandemics, extreme weather events, industrial accidents, and glacial melts) strikes converting into disasters in India. Each of these disasters is a gray rhino event that resulted in a large loss of life. The real disaster is India’s failure to recognise the early warning signs of these events and act proactively to save lives. A few of the recent major gray rhinos are:
-
Bhopal gas tragedy, 1984: Journalist Rajkumar Keshwani’s articles warning that the Union Carbide’s Bhopal plant was rundown and prone to a catastrophic accident went unheeded. The toxic gas that leaked from the plant is responsible for over 25,000 deaths till date.
-
Ersama cyclone, 1999: The National Remote Sensing Agency’s satellites tracked the Ersama super cyclone and warned of its intensity and landfall location, which were ignored. This resulted in 50,000 deaths in Orissa.
-
Bhuj earthquake, 2001: The earthquake resistant codes for engineered and non-engineered structures prepared by the Bureau of Indian Standards were never enforced in Bhuj and surroundings, a Category 5 (maximum risk) seismic zone. In the 7.5 magnitude earthquake that hit Bhuj, houses collapsed like a pack of cards, killing 25,000 people.
-
Indian Ocean tsunami, 2004: A 9.1 magnitude underwater earthquake epicentered off the Sumatra coast triggered a tsunami that hit the Andaman Islands at 7 am. The Indian government was immediately informed and had two hours to evacuate the India’s east coast before the tsunami reached it. No action was taken resulting in the death of 10,000 fisherfolk in Tamil Nadu and Andhra Pradesh.
-
Extreme weather events: Climate scientists have been warning that the frequency and intensity of extreme weather events would rise, yet India has remained unprepared. Some of the extreme weather events that occurred recently are--heavy rainfall: Mumbai, 2005 (deaths--1,000), Kedarnath, 2013 (5,000), Chennai, 2015 (500), Kerala, 2018 (500); heat waves: all over India, 2018 (2,400).
If Sun Tzu’s (Chinese general and military strategist, 50 BC) teaching, “If you know the enemy (gray rhinos) and know yourself (India’s capacity to deal with major hazards), you need not fear the result of a hundred battles” is continued to be ignored, India may well earn the name apadadesh (Disasterland).
Low Value for life
India lacks good risk mitigation programmes as it is a low-value and a low-price-of-life society. Value of life is the extent to which society nurtures and supports every person’s life regardless of identity. High value-of-life societies minimise risk from disease, violence, natural and manmade hazards, hunger, deprivation, poverty and all other stresses.
Giving life a price is likening it to a commodity. High price-of-life countries give large compensations for wrongful injury or death. Many North nations are high-price-of-life societies even though they are not high-value-of-life societies.
India’s transition to becoming a high value-of-life society must be by becoming a high price-of-life country first, and this transition should be led by the government. The ground for this exists in the 1985 Bhopal Gas Act, which is based on the legal doctrine parens patriae. The doctrine confers the state with the power to act as the guardian of those who cannot care for themselves. The Supreme Court of India has broadened the scope of this doctrine by stating, “Court has also a duty under the doctrine of parens patriae to take care of the rights of animals since they are unable to take care of themselves."
Having accepted the parens patriae doctrine, the government must provide free universal vaccination well within the next one year (at the current rates, it will take two and a half years to vaccinate India’s adult population), and ramp up public healthcare infrastructure by setting up temporary COVID care centres. This will ensure that another catastrophe is not repeated in subsequent COVID-19 waves.
The state’s basic duty is to look after the welfare of all its citizens, and public health is central to this duty. If the state is negligent in performing its duty, it must compensate for injury and death. The Indian government used the Bhopal Gas Act to go to the US courts to seek compensation a per US norms. It should therefore pay compensation per US norms for negligent deaths that it has caused. If compensation for wrongful death in the US is $10 million per death, the equivalent amount payable in India is Rs 35 million (computed at 2020 exchange and PPP rates). If we consider only the 170,000 reported COVID-19 deaths during second COVID-19 wave, 14 Feb-29 May 2021, is due to government’s negligence, the compensation payable is Rs 6 trillion. If all 326,000 reported deaths till date are considered, the amount is Rs 11.4 trillion.
The transition from a high price-of-life society to a high value-of-life society in India, a country that imbues the spirit of vasudhaiva kutumbakam (the world is one family), requires deep social changes and greater time.
Reducing Gap between Actual and Perceived Risk
The government’s underassessment of the coronavirus risk is one of the primary reasons for the erratic decisions taken during the pandemic. The gap between the actual and perceived risks is not unique to COVID-19, but has happened in every major hazard strike in India, and consequently, the country has mismanage them.
India’s sluggishness in tackling major hazards strikes is a systemic problem that requires a systemic solution. The government and people must exert mutual pressure on each other to close the gap between actual and perceived risk from major hazards and become more responsive to them. For this government must learn to cooperate with people rather than command them, collect and share good information on the major hazards, and hold dialogue with the public on its risk mitigation policy.
India is in one of the most vulnerable regions to global warming impacts. In the near future India will be battered by extreme weather events, sea rise, glacial melts, heat stress, water and food shortages, biodiversity loss and increase in vector borne diseases. Over eighty critical non-renewable minerals, including fossil fuels and other common metals, will be exhausted within this century. India must prepare from now to face these challenges by changing its outlook from “gain maximisation for a few” to “risk minimisation for all.” As a first step, India must make three parametres—good environment, food and water security, and health security—fundamental rights, and allocate 10% of the Union and state government budgets for each of them.
(The author is a risk analyst. He was a consultant to UNEP, Director (Safety), Envirotech Consultants Pvt Ltd, and faculty at BITS, Pillani. Views expressed are personal.)
Get the latest reports & analysis with people's perspective on Protests, movements & deep analytical videos, discussions of the current affairs in your Telegram app. Subscribe to NewsClick's Telegram channel & get Real-Time updates on stories, as they get published on our website.















